Story
 August 7, 2025
August 7, 2025
U.S. Helped Beat Back Malaria in Guinea. Now, the Disease Is Set To Soar
Country:



The effects of these cuts on the well-being of children


The Pulitzer Center's support for this reporting was made possible through the Stavros Niarchos Foundation (SNF) and the Gates Foundation.
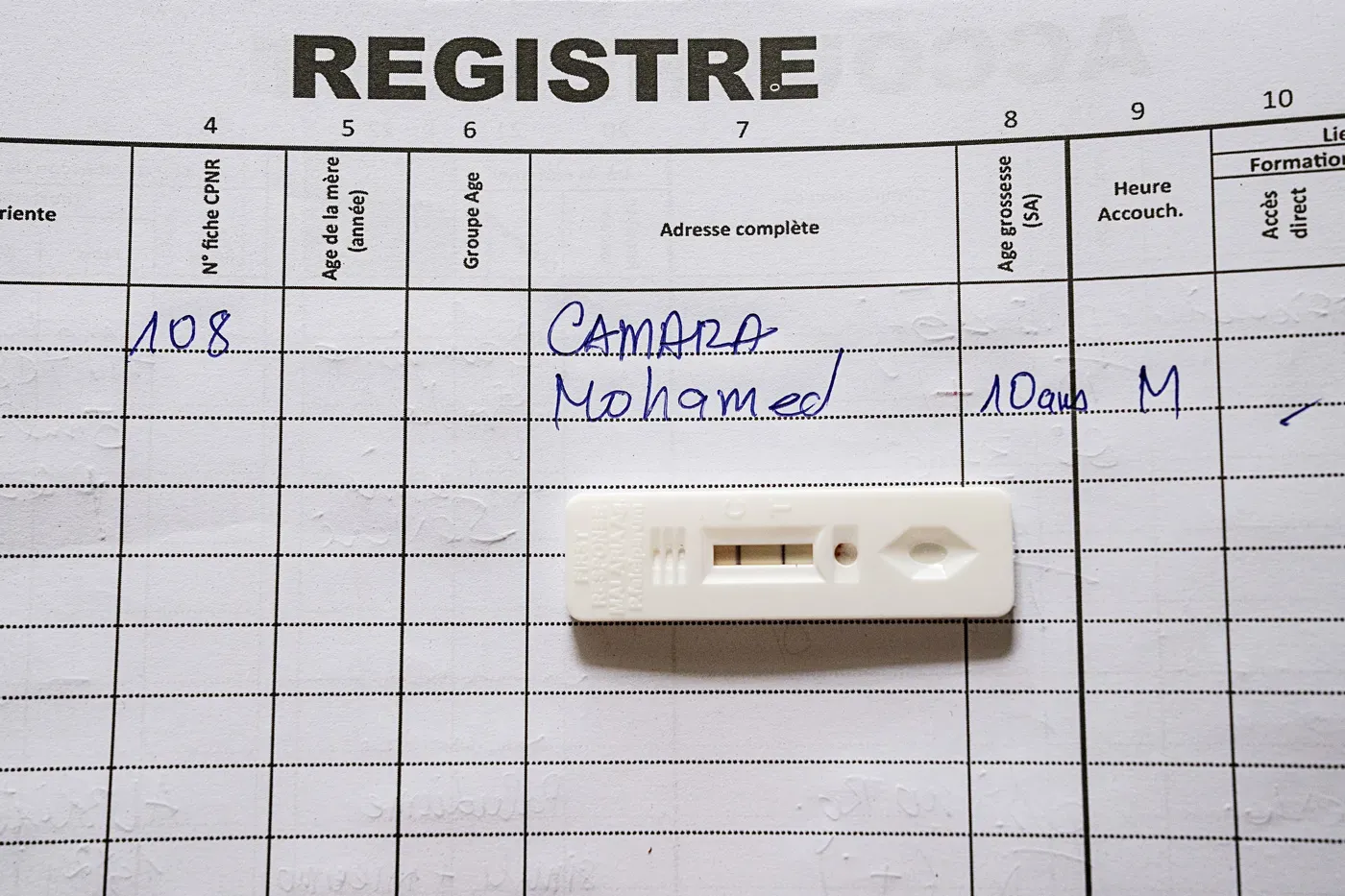
One morning in mid-June, a 10-year-old boy named Mohamed Camara was lying on a bed in a health center in the small Guinean town of Tamita, wearing bright blue shorts and an army-style T-shirt with Chinese characters on it. He looked listless and feverish; little pearls of sweat flowed from his forehead. He had just been diagnosed with malaria.
That morning, Mohamed’s parents had taken him to the center, which sits about 20 kilometers from the Atlantic coast in Boffa prefecture. Now, they and his baby sister were sitting on the bed next to him, looking anxious. “We were very worried,” said his father, Alseny Camara. They would have brought their son to the hospital earlier, he noted, but his job as a driver had taken him away from home for a few days.
Just 6 months earlier, Mohamed’s parents would have been able to call a community health worker when he got sick. That person might have come to the Camaras’ home on a motorcycle, taken a drop of blood, and applied it to a rapid diagnostic test, which looks a lot like a home test for COVID-19. After the thin line indicating a malaria infection had appeared, the health worker would have given the boy a first dose of drugs and explained to his parents how to continue the treatment. (If his symptoms were severe, Mohamed would have been referred to the health center instead.) A few days later, the worker would have checked in to see how Mohamed was doing.

As a nonprofit journalism organization, we depend on your support to fund more than 170 reporting projects every year on critical global and local issues. Donate any amount today to become a Pulitzer Center Champion and receive exclusive benefits!
Community health workers—laypeople trained to provide a few primary health services—are an essential part of the medical system in many African countries, and they’re particularly important in the fight against malaria, when a few days’ delay in diagnosis and treatment can make the difference between life and death. In Guinea, where the country’s entire population of more than 14 million is at risk of malaria, thousands of these workers lost their jobs after the United States suddenly froze billions of dollars in foreign aid in January, just days after President Donald Trump took office.

Mohamed was lucky his parents were finally able to bring him in—and that he did not have a severe case of the disease, which is caused by a mosquito-borne parasite that can infect the brain and cause life-threatening anemia and organ failure. Once at the health center, he was put on artemether-lumefantrine, the standard drug combination for malaria. He would be fine, said his doctor, who later sent Science a text message confirming the boy had been discharged. But other parents may not have the means to get their child to a doctor—or not in time, said the center’s director, Aïssata Camara. (She was not related to the boy; many people in this part of Guinea have the family name Camara.)

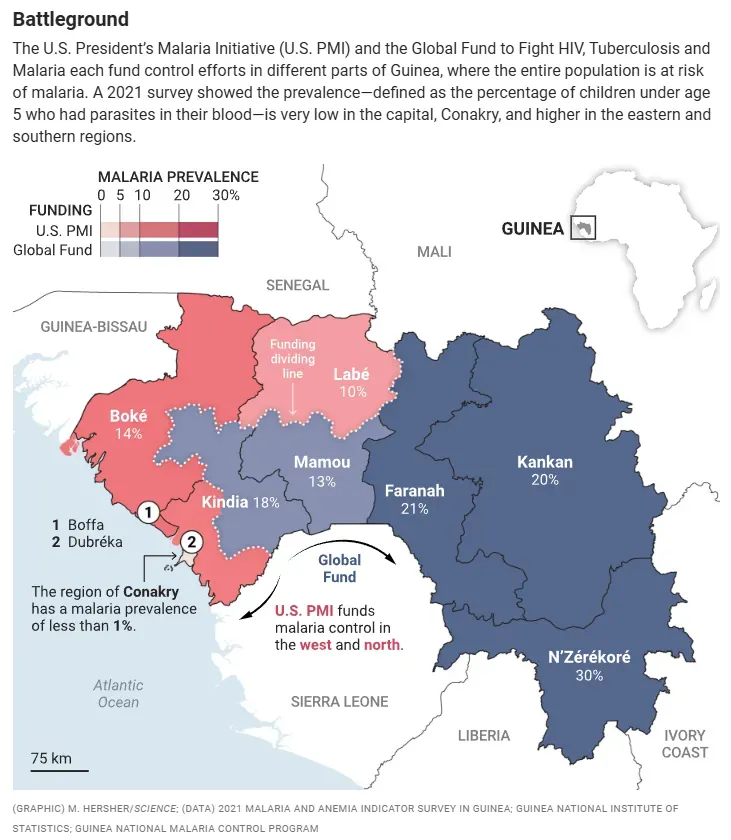
The disruption in U.S. funding for malaria control in Guinea—which amounted to some $15 million in 2024—has interrupted or put at risk many other health services in the West African nation, including the provision of diagnostic tests, drugs, and long-lasting insecticidal bed nets, as well as data collection, technical support, and training. The Trump administration has terminated much of the work of the President’s Malaria Initiative (PMI), launched 2 decades ago, which funded malaria control efforts for roughly half the Guinean population, including the bustling capital, Conakry. The U.S. has also threatened to dial down its contribution to the Global Fund to Fight HIV, Tuberculosis and Malaria, which funds efforts in the remainder of the country (see map, below).
There is no doubt Guinea will see malaria cases and deaths rise as a result, says Nouman Diakité, monitoring and evaluation manager at the country’s National Malaria Control Program (NMCP). “That has already started,” he says. Cases in Guinea spike during the rainy season, between late May and November, when mosquito populations soar. As always, children under age 5—who account for about three-quarters of malaria deaths—and pregnant women will be hardest hit, Diakité says.
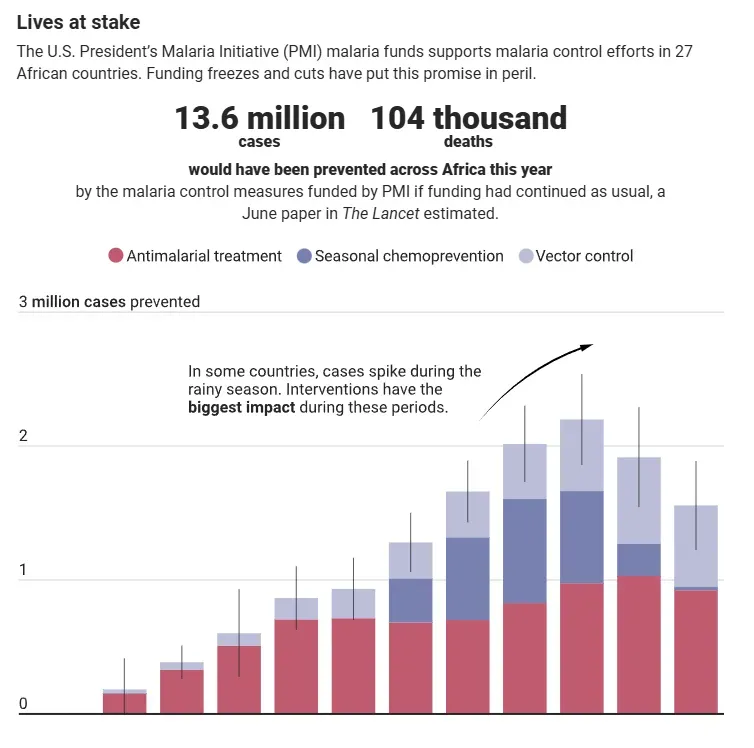
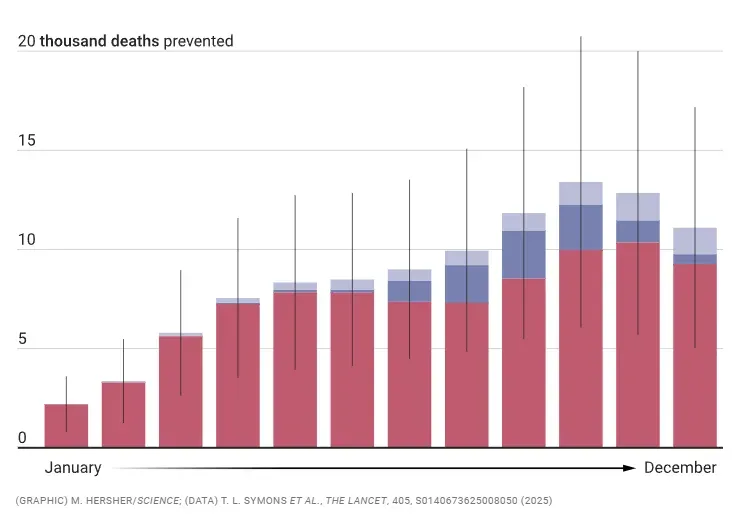
Malaria surges are also expected across the dozens of other countries where PMI has provided support, but the scale of the toll is hard to predict. In a modeling paper published in The Lancet in June, researchers at the Australia- and Tanzania-based Malaria Atlas Project estimated that if PMI had continued as usual, it would have prevented 13.6 million malaria cases and 104,000 deaths across sub-Saharan Africa this year, including 250,000 cases and 450 deaths in Guinea (see graphic, below.)
Not all of those gains will be lost, as some U.S. funding for malaria is continuing. The U.S. Agency for International Development (USAID), where PMI was housed, has been dissolved and about 95% of its more than 10,000 employees were laid off. But in a 25 July email to Science, a spokesperson for the U.S. Department of State said it is “committed to ensuring a smooth integration of designated life-saving global health programs from USAID to the Department and this transition is well underway.”
Countries are also trying to replace U.S. funding, and Guinea has bagged a few donations from nongovernmental partners. But they can make up just a tiny fraction of what’s gone. And whatever the immediate impact of the cuts, public health experts expect malaria cases to soar in the coming years, as flagging mosquito control efforts allow malaria transmission to rebound. “Unfortunately, we may see some natural experiments on how rapidly things can evolve,” says Regina Rabinovich, former head of the Gates Foundation’s infectious diseases division and a scholar in residence at the Harvard T.H. Chan School of Public Health. “It’s a tragedy.”
In Guinea, health officials, scientists, and staff at health facilities told Science they felt abandoned by a once reliable partner. Alhassane Camara, a community health worker in a town named Keleya, was still wearing a polo shirt and a vest emblazoned with American flags and the red, white, and blue USAID logo, along with the agency’s friendly tag line: “From the American people.” But he had lost his income—about $50 a month—and his motorcycle, and although he was still helping families close to his home, it was no longer possible to reach those farther afield.


Tears welled up in Camara’s eyes as he talked about the past 6 months, and in an emotional outburst, he suddenly switched from French, Guinea’s official language, to halting English. “I beg Donald Trump! People are gonna die!” he shouted. “The small children, they die!”
The U.S. has played an outsize role in the global fight against malaria for 2 decades. It provided more than $1 billion in bilateral funding for the disease in 2024, making it the largest government donor by far. In addition, the U.S. provides roughly one-third of the budget of the Global Fund.
That largesse began during the presidency of George W. Bush. PMI was launched with strong bipartisan support in 2006, with an initial $30 million to support malaria programs in Angola, Tanzania, and Uganda. It marked the advent of a golden era for malaria control, says Richard Steketee, who was PMI’s deputy U.S. global malaria coordinator from 2018 to 2023. The Global Fund, launched in 2002, was growing rapidly, the World Bank began to make funding available for malaria in 2005, and Bill and Melinda Gates made the disease a priority for their philanthropic organization. In 2007, the couple even called for malaria to be eradicated, reviving a broken dream from the 1950s.
Major strides seemed possible. In the 1990s and early 2000s, insecticide-treated bed nets had been convincingly shown to slash cases and deaths. A new group of very effective drugs named artemisinin-based combination therapies—including the one that cured Mohamed—had replaced older medicines to which Plasmodium falciparum, the most deadly malaria parasite, had become resistant. (Resistance against the combinations has emerged, primarily in Southeast Asia, but they have by and large retained their potency in Africa.) Rapid diagnostic tests made it possible to detect cases earlier and even in very remote places where the classic method—looking for parasites in the patient’s blood using a laboratory microscope—isn’t feasible.


PMI started procuring nets, tests, drugs, and insecticides for indoor spraying in large quantities and helping countries set up systems to distribute them and monitor whether they curbed malaria transmission. For the first time, Steketee says, “We were talking about scaling up coverage in order to achieve impact.” PMI’s budget grew to nearly $800 million in 2024, supporting 27 countries in sub-Saharan Africa and three more in Southeast Asia that together account for 90% of malaria cases and deaths.
One of those hot spots is Guinea, which had an estimated 4.4 million cases and more than 10,000 deaths in 2023, according to the World Health Organization’s (WHO’s) World Malaria Report 2024. More than half the population lives below the national poverty line and health services are rudimentary. Each year when the rainy season swells puddles and ponds, Anopheles mosquitoes swarm and bite, and feverish patients fill clinics. Most adults have had repeated bouts, gradually building up immunity against the disease. But children, whose immune systems have not learned to fight the parasites, are at much greater risk. In 2005, roughly one of every six children born in Guinea died before they turned 5 years old, many from malaria.

U.S. assistance soon began to change the picture. Thanks to the combined efforts of PMI and the Global Fund, insecticide-treated bed nets, virtually absent 20 years ago, have been introduced widely and are being replaced every 3 or 4 years in large campaigns. In regions where malaria is highly prevalent and seasonal, more than 1.1 million children under age 5 are now given antimalarial drugs monthly during the peak transmission season, a strategy called seasonal chemoprevention that helps avert infection and disease. About half of the country’s pregnant women—whose immune systems are temporarily weakened—get at least three doses of a combination antiparasitic drug named Fansidar, which protects the mother from malaria and reduces the risk of spontaneous abortion, stillbirth, premature delivery, and low birth weight.
In contrast to Guinea’s programs for HIV and tuberculosis, its malaria effort kept running—with extra safety precautions—during West Africa’s horrific 2013–16 Ebola epidemic, which killed more than 2500 Guineans. “That was a point of great pride,” says Richard Reithinger, a former distinguished research fellow at RTI International, a nonprofit based in North Carolina that implemented the PMI-funded programs.
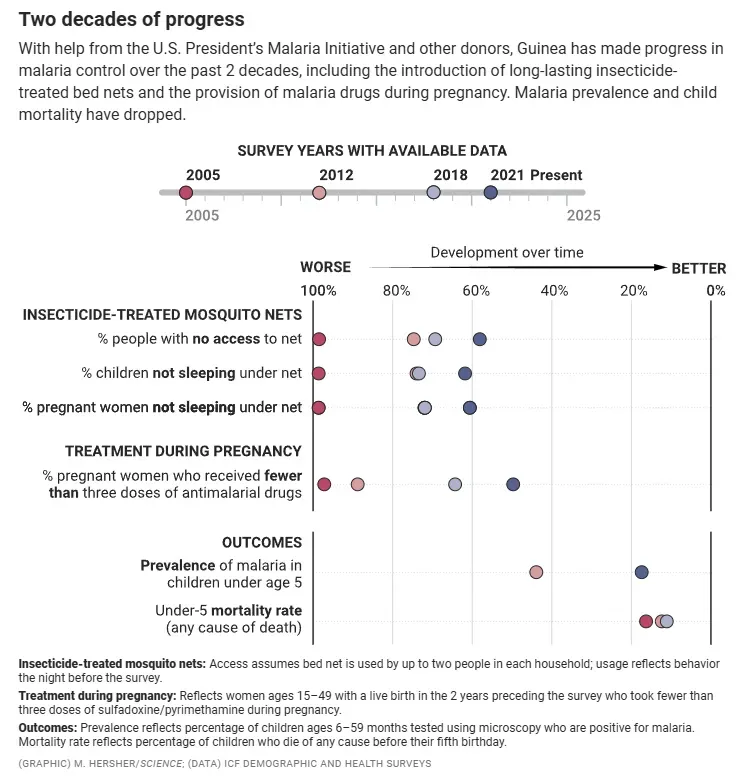
Measuring the programs’ success is not straightforward. In most African countries, many malaria cases and deaths occur at home and aren’t reported. One key indicator, however, is malaria prevalence, typically measured as the percentage of randomly sampled children between 6 months and 5 years of age confirmed to have malaria parasites in their blood. In Guinea, that number dropped from 44% in a 2012 nationwide survey to 17% in 2021—although there was huge variation between regions, with some reporting a prevalence of up to 30%. Child mortality dropped by one-third between 2005 and 2018. “Guinea has really made tremendous progress,” Reithinger says.
The collapse came as a complete surprise. Rumors started to circulate soon after Trump ordered a 90-day pause on foreign aid in an executive order signed on Inauguration Day, says Alioune Camara, NMCP’s coordinator. Soon after, Guinea was told to stop USAID-funded activities. Camara tried to contact USAID staffers at the U.S. embassy. “I’m not allowed to tell you anything,” he was told. Eventually, all the USAID employees were repatriated to the U.S.
Chaos and uncertainty have reigned since. After a review by the State Department—and a leaked USAID memo in March that warned of the devastating death toll if all foreign aid were ended—the department unfroze some “life-saving” malaria funding, including for drugs and bed nets. But analysis by KFF, a U.S nonprofit focused on health policy, found 80% of the 157 USAID contracts that included malaria activities were terminated.
RTI International laid off almost its entire local staff in Guinea, some 60 people, Reithinger says. The organization—whose biggest client is the U.S. government—also laid off hundreds of U.S. employees, including Reithinger.

During an interview at his office 6 months later, Ibrahima Kankalabé Diallo, the top health official in Boffa prefecture, ticked off a list of 15 things the U.S. had supported that had come to a standstill or were at risk. They included paying community health workers, 378 in his district alone; the provision of essential medicines, computers, microscopes, and motorcycles; monthly meetings with the directors of the prefecture’s health centers; an ambulance; and a high-level gathering on World Malaria Day to raise awareness and keep the disease on the political agenda. “Nothing is like it was before,” Diallo said.
Fakouma Camara, a biologist based in Boffa, was one of only five Guinean experts certified by WHO to do malaria diagnosis using microscopy, thanks to training provided by PMI. He had gone on to work for RTI International as a trainer, teaching community health workers across the country how to use rapid diagnostic tests and lab technicians how to do microscopy. Camara gave Science a copy of a poster he had presented at last year’s annual meeting of the American Society of Tropical Medicine and Hygiene in New Orleans. It showed that two cycles of “supportive supervision” could help improve diagnostic practices at local labs.

Now, he was without a job and the training program had collapsed. “It’s horrible,” Camara said. “People talk a lot about medicines, but diagnosis is very important as well. You can’t eliminate malaria if you don’t do it properly.”
Concerns mounted at the beginning of the rainy season. At the prefectural hospital of Dubréka, about an hour outside of Conakry, more than half of all admissions in June were for malaria. The chief pharmacist there, Alpha Baldé, showed Science to a storage room with dwindling stacks of boxes with the USAID logo on it. They contained antimalarial drugs—and Baldé was worried they would not be replenished.
Guinea is hardly alone. In April, a WHO rapid assessment found that more than half of the 64 malaria-endemic countries had experienced moderate or severe disruptions to malaria services. According to an online dashboard run by the Roll Back Malaria partnership, seven countries now only have a 3-month supply of rapid diagnostic tests left; five only have enough artemisinin-based combination therapy for 3 months. “There is a panic in many countries,” says Maru Aregawi Weldedawit of WHO’s Global Malaria Programme.

Reithinger says he expects the biggest problems in countries such as Nigeria, the Democratic Republic of the Congo (DRC), Ethiopia, and Mozambique, where the malaria burden was already high and funds for controlling the disease were insufficient even before the U.S. cuts. “Those are countries where I would expect increases in malaria incidence to be observed following this year’s transmission season,” he says.
The growing toll will be difficult to track because so many cases and deaths aren’t counted to begin with. PMI funding helped countries collect data and ensure their quality, and its loss has added to the challenge. And in February, the Trump administration killed the USAID-supported Demographic and Health Surveys Program, which collected vast amounts of health data—including on malaria—every few years in more than 90 developing countries. “We’re essentially going to be flying blind,” Alioune Camara said.
The future of U.S. support for malaria control is unclear. In its email to Science, the State Department stressed, “PMI’s key life-saving activities in malaria prevention and treatment are continuing.” It said at least 10 contracts were still providing commodities to PMI partner countries, including more than 3 million insecticide-treated bed nets in the DRC and Ethiopia and seasonal chemoprevention for more than 7 million children in West Africa.
Global health leaders were somewhat heartened in late July when a key spending panel in the House of Representatives—in a rebuke to the Trump administration—voted to maintain funding for many global health programs, including for malaria, at this year’s levels. But whether the bill will become law is uncertain, and even if it does, many worry that, with the existing aid structure torn to shreds and thousands laid off, the State Department will have to reinvent the wheel. “The mechanisms for that support have all been disbanded,” Steketee says. “There is nobody in the countries to actually do any of the local contractual and field support work.”

The fate of the Global Fund is also murky, as the U.S. and other countries reduce their commitments. Uncertainty about its financial future has recently led the fund to scale back many previously awarded grants. In late June, Alioune Camara learned the fund’s $81.5 million in support for malaria control in Guinea in 2024–26 would be cut by 9.4%. The country’s HIV and tuberculosis programs saw similar reductions.
But there have been glimmers of hope for Guinea. GiveWell, a U.S. charity with a strong focus on cost-effectiveness, has pledged up to $560,000 to RTI International to avoid delays in this year’s seasonal chemoprevention campaign, an approach GiveWell rates as highly cost-effective. The group has made donations to support the strategy in Mali, Cameroon, Ivory Coast, Togo, and Benin, reaching a total of 4.5 million children. Still, says GiveWell program officer Natalie Crispin, the group doesn’t want to create the impression it can replace the vast sums the U.S. government provided: “It’s a really challenging communication to get right.”
In a similar vein, the Against Malaria Foundation, which has provided Guinea with bed nets since 2019, has agreed to pay $1.8 million to ensure 4.8 million nets were distributed in July in spite of the U.S. funding freeze. Two other groups together chipped in another $900,000. (In the end, the U.S. government continued to fund bed net distribution in Guinea after the USAID freeze.)

Low- and middle-income countries may also have to start spending more of their own money on malaria control. “Domestic resource mobilization,” in global health parlance, has been on international agendas for many years, but the recent upheaval has given the discussion a fresh impetus. “Many countries have become heavily dependent on external funding,” Weldedawit says—even those that could shoulder more of the burden themselves.
Guinea, for example, is rich in resources and one of the world’s biggest bauxite producers. If only 1% of that industry’s proceeds were used for health, the country could take care of malaria control itself, says Alioune Camara, who has made that case to the government. “Will they? That is the big question now.”
Reithinger is “cautiously optimistic” about Guinea’s future. Although the U.S. cuts will have an impact, “I think we have a tendency to underestimate country governments,” he says. “I do know the Guinean health system, and I’ve seen how they have weathered and come out of the Ebola crisis, and how they managed the COVID crisis. … I think there is tremendous resilience in the system.”
People on the ground are far less sanguine. At the Tamita health center, where new malaria patients arrived almost daily, too many things were falling by the wayside, said Aïssata Camara, the center’s director. “The continuity is in danger,” she said. “We want American support to come back.”


